Compulsive Buying Disorder — I’m Trying to Understand
An accessible, evidence-based exploration of compulsive buying and shopping — what the research currently shows, why this area is genuinely complex, and how clarity may help.
Why understanding matters
Shopping is woven into nearly every part of modern daily life — acquiring necessities, marking occasions, pursuing interests, and navigating an economy built around consumer choice. For most people, buying things is simply a practical and occasionally enjoyable activity.
Yet for some people, their relationship with buying begins to feel less like a choice and more like a compulsion. Financial harm accumulates. Relationships are affected. Mood shifts in ways that are temporarily managed by purchasing and then worsened by the guilt that follows. The behavior continues in ways that feel difficult to control, even when the person recognizes the cost. This experience — when it reaches that point — is real, clinically meaningful, and worth taking seriously.
Understanding what the research says matters because the public conversation has often swung between two unhelpful extremes: dismissing it as simply a matter of poor financial discipline, or uncritically adopting the language of addiction without examining what that framing does and does not explain. Neither position reflects what the science actually shows. What the evidence reveals instead is a more nuanced picture: a behaviorally significant phenomenon whose psychological architecture is increasingly well-described, whose formal diagnostic status remains genuinely unsettled, and whose relationship with other mental health conditions is central to understanding it well.
What is meant by "compulsive buying disorder"?
Compulsive buying disorder — also described in the research literature as buying-shopping disorder or shopping addiction — describes a pattern in which buying has shifted from voluntary and functional to something more driven and impairing. It is not a formally codified diagnosis in DSM-5 or ICD-11. The term is used in research and clinical settings to describe a behavioral profile that is well-recognized in the literature, without overstating what the current science officially supports.
A critical distinction runs through all serious research in this area: the amount spent is not the right measure of whether buying is problematic. What matters is not the sum — it is motivation and consequence. Why is the person buying? What is being displaced? Is the pattern causing demonstrable harm to finances, relationships, mood, or daily functioning? Without functional impairment, the concept of compulsive buying does not apply.
Classification note: CBD currently has no formal code in DSM-5 or ICD-11. This reflects the ongoing process of reaching consensus on standardized criteria — not scientific doubt about whether the condition exists or causes harm. Clinicians can document CBD under applicable residual categories in both systems while formal classification criteria continue to develop.
Key Distinguishing Features
- Difficulty regulating buying behavior despite wanting to cut back
- Buying organized around escape from aversive feelings rather than genuine need or enjoyment
- A recognizable emotional cycle: distress drives urge, purchase provides brief relief, guilt and remorse follow
- Preoccupation with shopping — persistent mental engagement with buying when not shopping
- Continued behavior despite visible negative consequences
- Escalation over time — needing to buy more frequently or spend larger amounts to achieve the same effect
- Concealment of purchases or financial information from others
- Not explained by heavy or frequent spending alone — impairment is the defining criterion
The spectrum of buying behavior
Buying behavior exists on a continuum. The overwhelming majority of people who spend heavily fall well within the range of functional engagement. Understanding this spectrum prevents both the under-recognition of genuine difficulty and the over-pathologizing of ordinary consumer behavior.
Functional Spending
Buying oriented around genuine need, enjoyment, or considered choice. Regulated and purposeful. No meaningful displacement of other life domains.
Heavy Engagement
Frequent or high-volume spending. May include enthusiasm for shopping as an activity. Not problematic when motivation is purposeful and functioning is preserved.
Emerging Concern
Buying beginning to serve escape or avoidance functions. Some slippage in financial management or mood following purchases. Full impairment not yet established.
Compulsive Buying
Persistent difficulty moderating buying. Organized around avoidance of internal distress. Demonstrable harm across financial and relational life domains. Impairment rather than mere intensity.
4–6%
How common is compulsive buying?
A 2016 meta-analysis by Maraz and colleagues — drawing on 40 studies and over 150,000 participants — estimated general population prevalence at roughly 4–6%. This means a meaningful minority of adults experience buying patterns that cross the threshold into genuine impairment. Prevalence estimates vary significantly depending on whether strict functional impairment criteria are applied.
CBD is more frequently identified in female populations in most research samples, though male underreporting is a recognized limitation. Age of onset is typically late adolescence to early adulthood. Movement along the continuum can occur in either direction — heavier spending during a stressful period does not automatically indicate a persistent pattern.
Pathways toward compulsive buying
Research has identified several recurring patterns in how buying can shift from purposeful engagement toward something more compulsive and difficult to regulate.
Reward Reinforcement and the Buying Cycle
Shopping activates reward circuitry in a way that is genuinely reinforcing. The anticipation of a purchase can itself produce hedonic engagement, and the act of buying produces a transient sense of relief or pleasure. What makes this pattern capable of becoming compulsive is what happens after: the relief is brief, rapidly replaced by guilt, remorse, and a return to the original negative emotional state. This negative-positive-negative cycle is the functional mechanism through which compulsive buying becomes self-reinforcing over time. Repeated engagement under these conditions appears capable of producing neuroadaptation, driving escalation in frequency, spending amounts, or novelty to achieve the same effect — paralleling tolerance dynamics observed in other behavioral patterns.
Avoidance Coping and Its Long-Term Consequences
One of the most clinically significant pathways involves turning to buying as a way of managing or escaping uncomfortable internal states — anxiety, sadness, shame, loneliness, or a diffuse sense of inadequacy. This works in the short term. The problem that develops over time is that when someone consistently turns away from difficult feelings by buying rather than processing them, the capacity to tolerate those feelings gradually diminishes. Over time, buying may become the primary available strategy for managing emotional distress — making the cycle progressively harder to interrupt.
Self-Esteem, Identity, and Materialism
Individuals who develop compulsive buying characteristically present with low baseline self-esteem and a compensatory orientation toward materialism — a tendency to seek in acquisition something of what is missing in their sense of their own worth. Consumer culture actively reinforces this connection. This susceptibility is not a character flaw; it reflects an identifiable pattern of psychological vulnerability that is amenable to support.
Impulsivity and the Gap Between Urge and Control
Elevated impulsivity — the tendency to act on urges without adequate deliberation or inhibition — is a reliably identified feature. The experience many people describe is not simply wanting things, but a mounting urge that available self-control cannot adequately contain. The disproportion between urge intensity and inhibitory capacity appears to be a more specific feature of the pattern than the urge alone.
Note: the neurobiological evidence specific to CBD is largely inferential. Current biological descriptions represent evidence-based inference from behavioral patterns rather than established mechanistic certainty from dedicated neuroimaging research.
The Digital and E-Commerce Environment
The contemporary online retail environment represents a materially distinct and increasingly significant pathway. E-commerce platforms are deliberately designed in ways that reduce the friction between urge and purchase: one-click checkout, 24/7 availability, algorithmic product personalization, push notifications, and seamless mobile access all systematically shorten the interval between impulse and action. For individuals who are not vulnerable to compulsive buying, these features are convenient. For those who are, they directly operationalize the conditions under which compulsive urges are most readily triggered and least likely to be interrupted. The role of digital retail design in both onset and escalation is increasingly documented in the research literature. If you or someone you know finds online shopping significantly harder to control than in-store shopping, that pattern is not coincidental — it reflects a meaningful interaction between individual vulnerability and environmental design. Recognizing this is practically useful: structural access restriction (deleting apps, removing saved payment credentials, imposing mandatory purchase delays) is among the most directly effective behavioral strategies available.
Practical note: Deleting shopping apps, removing saved card details, and establishing a mandatory 24-hour waiting rule before any non-essential online purchase are concrete first steps that directly interrupt the urge-to-purchase pathway — and require no clinical intervention to implement.
Primary concerns versus secondary patterns
One of the most important questions in this area — and one that directly shapes what kind of support is most helpful — is whether compulsive buying is a primary concern or whether it is better understood as a secondary expression of something else. Research suggests that in many clinical presentations, the latter is more common.
Depression and Mood
Mood disorders — particularly major depressive disorder and dysthymia — represent the most commonly co-occurring conditions in compulsive buying. Low mood drives acquisition as a coping strategy, and the guilt and financial consequences of compulsive buying can in turn deepen depression, creating a mutually sustaining cycle. Where significant depression is present, it is often doing much of the organizing work.
Anxiety
Anxiety disorders — including social phobia, generalized anxiety disorder, panic disorder, OCD, and posttraumatic stress disorder — appear with notable frequency alongside compulsive buying. For individuals managing persistent anxiety, buying may function as a reliable, immediately available source of relief. The anxiety-driven, ritualistic quality of the buying urge-and-relief cycle is one reason researchers have noted phenomenological overlap with OCD-spectrum presentations.
Anxiety
Anxiety disorders — including social phobia, generalized anxiety disorder, panic disorder, OCD, and posttraumatic stress disorder — appear with notable frequency alongside compulsive buying. For individuals managing persistent anxiety, buying may function as a reliable, immediately available source of relief. The anxiety-driven, ritualistic quality of the buying urge-and-relief cycle is one reason researchers have noted phenomenological overlap with OCD-spectrum presentations.
Eating Disorders
Binge eating disorder appears alongside compulsive buying with sufficient frequency to suggest possible shared mechanisms involving impulsive consumption and affective dysregulation. Both patterns involve episodic loss of control over a consumption behavior in response to aversive emotional states, followed by remorse. This overlap points toward the importance of thorough comorbidity assessment.
Substance Use and Other Behavioral Addictions
Substance use disorders and other behavioral addictions — including gambling — are significantly overrepresented among individuals with compulsive buying. The co-occurrence of multiple patterns organized around impulsive reward-seeking and affect regulation suggests a broader vulnerability to loss of control over reinforcing behaviors, rather than a narrowly specific susceptibility to shopping.
The practical implication: Where a primary condition can be identified — depression, anxiety, or another disorder — its treatment is a primary clinical act. Compulsive buying behaviors are anticipated to improve as the underlying condition is addressed. Directing effort exclusively at the buying behavior while leaving an organizing condition unrecognized is likely to produce only partial and temporary change.
What the current diagnostic landscape says
Compulsive buying disorder holds no formal diagnostic status in DSM-5 or ICD-11. This absence reflects genuine scientific caution rather than a dismissal of the clinical reality. Regulatory and scientific bodies require consensus on diagnostic criteria and course characterization that the evidentiary base has not yet produced. The absence from official classification should not be misconstrued as an absence of clinical significance.
Part of what makes compulsive buying conceptually complex is that it genuinely resembles several distinct disorder families without belonging cleanly to any of them. Its phenomenology overlaps with OCD and related disorders in the anxiety-driven, ritualistic quality of the buying urge-and-relief cycle. It parallels impulse control disorders in the failure to resist a mounting impulse despite awareness of harmful consequences. And it shares features — including loss of control and affective dysregulation — with behavioral and substance addictions. Most contemporary frameworks position it along an impulsive-compulsive continuum, placing it closer to the impulsive pole alongside pathological gambling.
For those seeking help now: The absence of a formal diagnostic code does not mean that effective support is unavailable. Clinicians can recognize, document, and treat CBD using current residual classification categories. If you are experiencing significant distress or impairment related to buying behavior, that is sufficient reason to seek professional support — a formal diagnosis is not a prerequisite for help.
Why this topic generates debate
Compulsive buying has occupied an uncertain position in psychiatric nosology for decades, generating genuine scientific discussion. Understanding why this debate exists is part of understanding the subject itself.
The case for taking it seriously: The functional consequences are real and well-documented — significant financial harm, relationship damage, accumulating debt, and a persistent cycle of distress and deepened guilt. The patient experiencing these consequences deserves a thoughtful clinical response regardless of whether a formal diagnostic label can be applied.
Legitimate classification concerns: A genuine ongoing discussion concerns how to delineate compulsive buying from closely related conditions, which disorder family it most closely belongs to, and whether the clinical presentations that fall under this label are sufficiently homogeneous to constitute a single disorder. The spectral ambiguity is not merely academic; it has direct treatment implications.
The role of digital consumer environments: Emerging discussions have raised questions about the role of e-commerce design, advertising, and online retail platform architecture in sustaining and intensifying buying behavior — particularly in individuals whose self-identity is insecure or whose sense of worth has become entangled with material acquisition. These environmental factors are increasingly recognized as clinically relevant and are an active area of research.
What research consistently agrees on — and what remains uncertain
Reasonably settled evidence
- Impairment — not amount spent — is the appropriate measure of whether buying is problematic
- Comorbidity with mood and anxiety disorders is common and clinically important
- In many presentations, compulsive buying is secondary to an underlying condition
- The emotional cycle (distress → urge → relief → guilt → return) is consistently described and clinically significant
- Low self-esteem and compensatory materialism are reliably associated features
- Elevated impulsivity — specifically the urge-control disproportion — is a consistent predictor
- CBT has the most structured evidence base among psychological approaches studied
- Treating the co-occurring condition often produces meaningful improvement in buying behavior
- E-commerce design features are clinically relevant maintaining factors
Genuinely uncertain
- Whether CBD constitutes a distinct disorder or a symptom cluster across several existing conditions
- The most appropriate diagnostic classification — impulse control, behavioral addiction, or OCD-spectrum
- Whether neurobiological patterns precede, follow, or interact with the behavioral pattern
- The genetic architecture, despite preliminary familial signals
- Whether the condition manifests differently across genders
- The long-term trajectory across the lifespan
- Generalizability of findings beyond Western, industrialized research contexts
- The most effective specific formats and components of intervention
What helpful support looks like
Cognitive Behavioral Therapy (CBT)
CBT is the best-supported approach for compulsive buying. It directly targets the emotional cycle driving the pattern — the aversive feeling, the urge to buy, the brief relief, and the guilt that follows — by building skills to interrupt that cycle and respond differently to difficult feelings.
CBT helps people identify and examine the thought patterns and beliefs driving problematic behavior — including beliefs that link buying with self-worth or with relief from distress — and develop more balanced perspectives and alternative coping strategies. It addresses practical behavior change, including recognizing high-risk situations and building financial self-management skills. CBT can be delivered individually, in groups, in-person, or via telehealth.
Group therapy merits particular attention because it offers something individual therapy cannot replicate: the experience of being understood by others who share the same struggles. Compulsive buying carries significant shame — group membership can disrupt the isolation and self-stigma that otherwise prevent help-seeking.
Addressing Underlying Conditions
Because compulsive buying is so often connected to underlying mental health conditions — depression, anxiety, and others — support frequently works best when those conditions are addressed directly. Effective treatment of an underlying condition often leads to meaningful improvement in the buying pattern.
Behavioral and Structural Modifications
Practical behavioral modifications directly support clinical improvement. Limiting financial access — through removal of credit cards, use of cash or debit only, deletion of shopping apps, removal of saved payment credentials, and structural barriers to impulsive online purchasing — reduces the behavioral opportunity for compulsive buying. Engagement in structured alternative activities, consistent physical exercise, regular sleep, and reduction of alcohol use may reduce the affective vulnerability that triggers buying urges.
Holding the complexity honestly
The public conversation about compulsive buying tends to oscillate between dismissal and moralism. The research does not support either position.
Oversimplification
“People who overspend just lack self-discipline or willpower.”
What the research says
Research consistently identifies compulsive buying not as a character failing but as a recognizable pattern involving affective dysregulation, elevated impulsivity, and low self-esteem. Moral framing rather than clinical understanding is one of the primary barriers to people seeking support.
Oversimplification
“Shopping addiction isn’t a real clinical concern — everyone likes to shop.”
What the research says
For a meaningful subset of individuals — approximately 4–6% by current estimates — the relationship with buying becomes genuinely distressing and impairing. The behavioral and psychological mechanisms are real and increasingly well-characterized.
Oversimplification
“Compulsive buying is just about the shopping — address the shopping, address the problem.”
What the research says
In many presentations, compulsive buying is secondary to an underlying condition — depression, anxiety, or another disorder — functioning as a coping strategy. Addressing the buying behavior while leaving an organizing condition unrecognized is likely to produce only partial and temporary change.
Oversimplification
“Because compulsive buying isn’t in the DSM, it isn’t a real problem.”
What the research says
The absence of formal diagnostic status reflects the state of the science — the lack of consensus on criteria that formal classification requires — not a judgment about clinical significance. The disorder produces demonstrable impairment and substantial psychiatric comorbidity. The absence of a label does not diminish the reality of the experience or the legitimacy of seeking support.
Take Action
Where to Go From Here
Understanding this area is a beginning, not an endpoint. Where you go from here depends on why you came.
If you need help
Resources, support options, and next steps for individuals concerned about their own relationship with buying or spending.
For professionals
Clinical resources, assessment frameworks, documentation guidance, and evidence-based treatment references for practitioners.
For loved ones
Guidance for family members and friends who are concerned about someone's relationship with buying and want to help thoughtfully.
Educational Foundation
Content on this page synthesizes information from peer-reviewed clinical and scientific literature on compulsive buying disorder, including published systematic reviews, epidemiological literature, clinical treatment research, and assessment instrument development and validation studies. The nosological positions of DSM-5 (American Psychiatric Association) and ICD-11 (World Health Organization) are represented accurately as of the time of writing. This field is in a state of active scientific development; findings and frameworks should be verified against current primary literature for clinical or policy application. This page is intended for educational purposes only and does not constitute clinical guidance. For clinical assessment or treatment, consult a qualified healthcare professional.
Optional Advanced Exploration
Go Deeper — The Clinical Science of Compulsive Buying & Spending
For readers who want to explore the evidence base, the mechanisms, and the diagnostic debates in greater depth. These modules examine compulsive buying from its definitional foundations through psychology, structural and environmental drivers, comorbidity, and clinical management — a condition that is clinically real, diagnostically unresolved, and increasingly shaped by the e-commerce environment. They are optional — the core information above stands on its own.
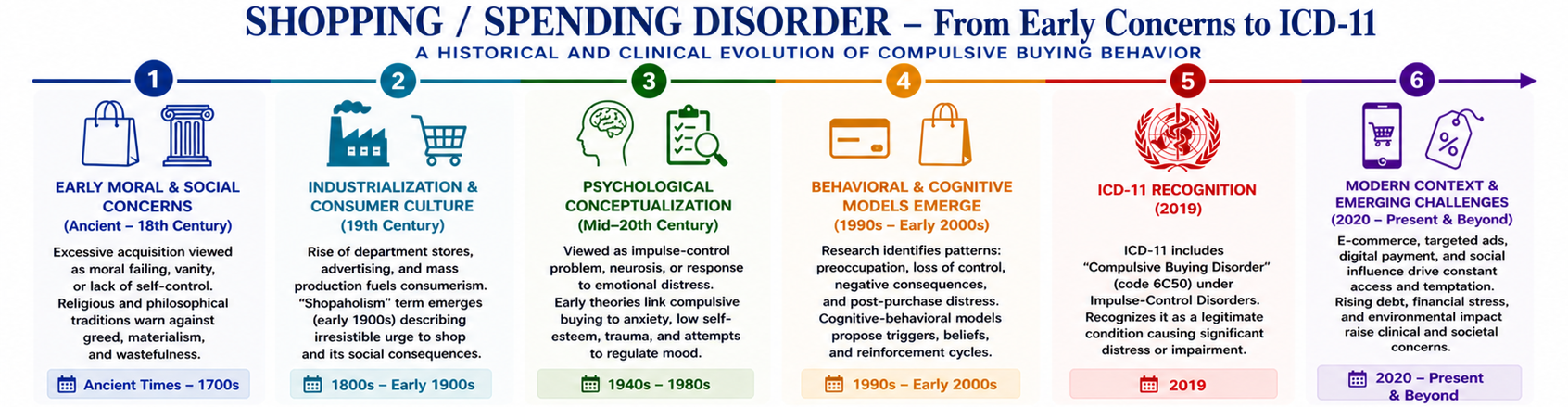
📊 Shopping / Spending Disorder – From Early Concerns to ICD-11: A Historical and Clinical Evolution of Compulsive Buying Behavior
Opening Orientation
A century of clinical recognition without a formal diagnosis — what compulsive buying is, why the diagnostic absence doesn’t reflect clinical insignificance, and how to engage honestly with the evidence.
The Definitional Problem
Where does shopping end and disorder begin? The Faber-O’Guinn definition, why prevalence estimates range from 1% to 16%, and what the risk of overdiagnosis requires clinicians to hold in mind.
Behavioral Phenomenology
The characteristic episode sequence, the dissociative quality that distinguishes compulsive buying from ordinary impulse purchasing, concealment behavior, and the amplified phenotype produced by e-commerce.
Psychological Mechanisms
The wanting-liking dissociation, negative reinforcement, mood regulation, identity and self-esteem functions, and the distinction between habitual and impulsive buying — each with direct treatment implications.
Structural & Environmental Drivers
Consumer credit, BNPL services, marketing psychology, and e-commerce architecture — the deliberately engineered structural conditions that enable and amplify compulsive buying at the individual level.
Psychiatric Comorbidity
Mood disorders, anxiety, ADHD, OCD-spectrum presentations, and binge eating disorder — why comorbidity is the rule, and the nosological debate that shapes how the condition is classified and treated.
Diagnostic Status & Controversy
No formal diagnostic home in DSM-5 or ICD-11. How to document these presentations, what the measurement problem has done to the evidence base, and the utility and risks of the “shopping addiction” label.
Clinical Approach & Management
Assessment priorities, CBT and DBT approaches, financial and environmental interventions, pharmacotherapy, and the treatment-goal question unique to a behavioral condition where abstinence is not viable.
Synthesis
Integrating biological, psychological, social, and environmental dimensions — and what calibrated clinical practice looks like for a condition whose mechanisms are increasingly understood but whose formal recognition remains incomplete.