Internet & Social Media Use — I’m Trying to Understand
An accessible, evidence-based exploration of internet and social media use — what the research currently shows, why this area is genuinely complex, and what has changed in clinical settings — particularly for adolescents — over the past decade.
Why understanding matters
The internet and social media are woven into nearly every part of modern daily life — work, relationships, information, identity, and recreation. For most people, digital technology is a genuine tool: enabling connection, productivity, and engagement. This is the ordinary experience for the vast majority of users.
Yet for some people, their relationship with internet use or social media begins to feel less like a choice and more like a compulsion. Sleep suffers. Relationships are affected. Mood and self-perception shift. The behavior continues in ways that feel difficult to moderate, even when the person recognizes the cost. This experience — when it reaches that point — is real, clinically meaningful, and worth taking seriously.
Understanding what the research says matters because the public conversation has often swung between two unhelpful extremes: dismissing it entirely as a matter of willpower, or treating any heavy use as evidence of addiction. Neither position reflects what the science shows. What the evidence reveals instead is a more nuanced picture: a behaviorally significant phenomenon whose mechanisms are increasingly well-described, whose diagnostic status remains genuinely unsettled, and whose relationship with other mental health conditions is central to understanding it well.
What is meant by "internet and social media use dysregulation"?
The phrase describes a pattern in which digital engagement has shifted from voluntary and functional to something more compulsive and impairing. It is not a formal diagnosis. The term is used in research and clinical settings to describe a behavioral profile without overstating what the science currently supports.
A critical distinction runs through all serious research in this area: time spent online is not the right measure of whether use is problematic. The same number of hours may represent productively necessary engagement for one person and a damaging pattern of escape for another. What matters is motivation and consequence — why is the person going online, what is being displaced, and is sleep, relationship functioning, mood, or daily performance affected in ways that cause real harm?
Classification note: Internet Addiction and Social Media Addiction currently have no formal code in DSM-5 or ICD-11. Internet Gaming Disorder appears in DSM-5 Section III as a condition requiring further study; Gaming Disorder is recognized in ICD-11. Clinicians can document these presentations under applicable residual categories while formal classification criteria continue to develop.
Key Distinguishing Features
- Difficulty regulating use despite wanting to cut back
- Use organized around escape from difficult feelings rather than purposeful engagement
- Sleep consistently displaced by late-night or nocturnal digital activity
- Preoccupation — persistent mental engagement with online activity when offline
- Continued use despite visible negative consequences
- Irritability or distress when unable to go online
- Erosion of functioning in relationships, work, study, or self-care
- Not explained by heavy or frequent use alone — impairment is the defining criterion
The spectrum of digital engagement
Internet and social media use exists on a continuum. The overwhelming majority of people who use digital platforms heavily fall within the range of functional engagement. Understanding this spectrum prevents both under-recognition of genuine difficulty and over-pathologizing of ordinary behavior.
Functional Use
Use oriented around work, relationships, interests, and recreation. Regulated and purposeful. No meaningful displacement of other life domains.
Heavy Engagement
Intensive, frequent, high-volume use. Not problematic when motivation is purposeful and functioning is preserved. Includes developmentally appropriate adolescent peer engagement.
Emerging Concern
Use beginning to serve escape or avoidance functions. Some slippage in sleep, relationships, or responsibilities. Full impairment not yet established.
Dysregulated Use
Persistent difficulty moderating use. Organized around avoidance of internal distress. Demonstrable harm across life domains. Impairment — not mere intensity — is the defining feature.
4–8%
How common is problematic internet use?
Estimated prevalence ranges from approximately 4–8% in general adult samples, with considerably higher estimates in adolescent populations — some studies report rates of 10–15% in adolescents using broadly defined criteria. These figures vary substantially depending on instrument and whether strict functional impairment criteria are applied.
Adolescents are consistently identified as the highest-risk demographic. Male users show higher rates of gaming-related patterns; female users show higher rates of social-media-specific patterns involving validation-seeking and social comparison. Both are clinically significant.
Pathways toward dysregulated use
Research has identified several recurring patterns in how internet and social media use can shift from purposeful engagement toward something more compulsive and difficult to regulate.
Reward Reinforcement and Platform Design
Social media platforms are built around one of the most powerful human motivations: connection with other people. Positive reactions online — a like, comment, reply — engage brain circuitry that overlaps with how other meaningful rewards are processed. What makes social media particularly compelling is the unpredictability of these rewards. Responses arrive at irregular intervals, which behavioral psychology has long established as the reinforcement pattern most likely to sustain repeated checking behavior — the same mechanism underlying slot machine behavior. This pull has a genuine neurological basis, not merely a volitional one. Brain imaging studies show differences in areas involved in self-control and reward processing — though these findings should be interpreted as evidence-based inference, not established mechanistic certainty, given that current research is largely cross-sectional.
Fear of Missing Out and Social Comparison
FOMO — a persistent, uncomfortable feeling that other people are having experiences or accessing information that one is not — drives compulsive monitoring of social environments. Social media intensifies this because what people share tends to be the highlights of their lives, carefully selected and more positive than everyday reality. Comparing oneself against these curated highlights can create the impression that everyone else is doing better, which drives further checking in a self-sustaining cycle. A second related pattern involves seeking reassurance through online activity — measuring self-worth in terms of social feedback. This can make a person's sense of themselves feel fragile and externally dependent. Research links this to perfectionism and anxiety — not as causes to be blamed, but as vulnerabilities worth understanding.
Avoidance Coping and Its Long-Term Consequences
The third pattern — and arguably the one with the most significant long-term consequences — involves turning to internet use as a way of managing or escaping uncomfortable internal states: stress, sadness, loneliness, boredom, or anxiety. This works in the short term. The problem that develops over time is that when someone consistently turns away from difficult feelings rather than processing them, the capacity to tolerate those feelings without reaching for a screen gradually diminishes. By the time this pattern is clinically apparent, the individual's unassisted tolerance for internal distress may be substantially reduced.
Sleep Displacement — Both Consequence and Cause
Sleep disruption is among the most consistently documented features of dysregulated internet use — and critically, it both results from and maintains the pattern. Late-night use displaces sleep time. Blue-light exposure from screens suppresses melatonin, interfering with natural sleep signaling. The knock-on effects of poor sleep — reduced concentration, greater difficulty managing emotions, lower mood, decreased self-control — are precisely the capacities needed to regulate internet use. Addressing sleep is often not a secondary concern but one of the most important starting points.
Platform Design as a Structural Maintaining Factor
Social media and internet platforms are deliberately engineered to maximize engagement time. Variable-ratio reinforcement schedules — the same mechanism driving slot machine behavior — underlie notification systems, like counts, and content feeds. Infinite scroll removes natural stopping cues. Algorithmic personalization surfaces content precisely matched to each individual's engagement history. These features are not incidental to the problem of dysregulated use — they constitute a maintained environmental substrate that systematically reduces the friction that would otherwise allow natural pauses between use episodes. These design choices are not inherently pathological for most users. But for individuals who are already vulnerable — whether through depression, anxiety, low self-esteem, or impulsivity — they directly operationalize the conditions under which compulsive use is most readily triggered and least likely to be self-interrupted. Understanding this removes the temptation to attribute dysregulated use entirely to individual character failure.
Recognizing the role of platform design is practically useful: structural modifications — turning off non-essential notifications, removing social apps from the home screen, using app time limits — directly interrupt the cue-to-use pathway and require no clinical intervention to implement.
Primary concerns versus secondary patterns
One of the most important questions in this area — and one that directly shapes what kind of support is most helpful — is whether problematic internet use is a primary concern in its own right, or whether it is better understood as a secondary expression of something else. Research suggests that in most clinical presentations, the latter is more common.
Depression and Mood
Depression and internet use sustain each other bidirectionally: low mood drives digital escape; digital escape impairs the sleep, social functioning, and self-regulatory capacity that would otherwise support mood recovery. Where depression is present, it is likely doing much of the organizing work in the pattern of use.
Anxiety and Social Anxiety
Anxiety — particularly social anxiety — appears consistently in research on problematic internet and social media use. For individuals who find face-to-face social situations demanding or threatening, online environments may offer lower-demand alternatives that become disproportionately preferred over time, reinforcing avoidance of real-world interaction.
ADHD
ADHD confers both the impulse inhibition deficits and the reward sensitivity that make prolonged digital engagement intrinsically reinforcing and difficult to moderate. The prevalence of ADHD among those presenting with internet use dysregulation is striking and consistent across multiple research populations.
Autism Spectrum Conditions
ASD, particularly in adolescence, may make the structured, predictable, low-social-demand environment of online interaction disproportionately rewarding relative to the ambiguous demands of face-to-face engagement. In these presentations, the online environment may be meeting a genuine need rather than functioning as simple escape — an important nuance for any access planning.
The practical implication: Where a primary condition can be identified — depression, anxiety, ADHD, or another disorder — its treatment is the primary clinical act. Directing effort exclusively at the internet use behavior while leaving an organizing condition unrecognized is likely to produce only partial and temporary change.
What is happening with adolescents — and why it matters
The past decade has brought a pattern of clinical presentations that has shifted how many professionals in adolescent mental health understand this topic. Understanding it matters for parents, educators, and anyone trying to make sense of what is happening with young people’s relationship with social media.
Adolescents represent the highest-risk group for problematic internet and social media use. This is not simply because they use these platforms more. It reflects a convergence of developmental factors that make them distinctively vulnerable: peer belonging is more psychologically central in adolescence than at any other life stage; identity is still being formed; the brain systems that regulate impulsive behavior are still maturing; and these converging developmental realities arrived at exactly the same moment as the mass adoption of maximally engaging social platforms.
Social media and identity in adolescence
For many adolescents today, social media is not simply a leisure activity — it is the primary medium of peer belonging, social identity, and real-time social standing. Being included in a group chat, having posts acknowledged, staying current with peers' social activity — these are not trivial concerns at this developmental stage. They are the substance of social life. Understanding this context is essential for understanding why the relationship with social media can feel so high-stakes for adolescents, and why interventions that would be manageable for adults can sometimes feel catastrophic to young people who are at a more vulnerable developmental stage.
Access restriction and acute psychiatric crisis
Clinicians working in adolescent inpatient and emergency psychiatric settings have been documenting a pattern over the past several years that deserves explicit public attention: adolescents presenting with suicidal ideation or self-harming behavior in the immediate aftermath of phone or social media access being removed — typically as a disciplinary consequence by parents or schools.
This pattern is worth understanding carefully. It does not mean that restricting access is always wrong. It means that for a subset of adolescents — those who are already psychologically fragile, whose primary source of peer connection is online, and who have not developed alternative means of affect regulation — abrupt and unilateral access removal can be a genuinely destabilizing event. The clinical response required in these situations is not simply restoration or escalation of the restriction, but comprehensive assessment of the young person's psychiatric state and the function that the access was serving.
If an adolescent in your care has expressed suicidal thoughts or engaged in self-harm — including in the context of device restriction — seek immediate professional support. Call or text 988, go to the nearest emergency department, or call 911 if there is immediate danger. The access question can be addressed thoughtfully once safety is established.
For parents considering restricting access
The instinct to restrict a young person's phone or social media access is understandable, and in some cases it may be the right decision. The evidence suggests that how this is done matters enormously. Restriction that is discussed in advance, implemented gradually, accompanied by clinical support, and attentive to what the device was providing the adolescent — peer connection, identity, a sense of belonging — is far more likely to produce positive outcomes than restriction imposed without warning or support. For adolescents who are already showing signs of significant emotional distress, consulting a mental health professional before implementing access restrictions is strongly recommended.
What research consistently agrees on — and what remains uncertain
Reasonably settled evidence
- Impairment — not time spent — is the appropriate measure of whether use is problematic
- Sleep disruption is among the most consistently documented consequences, and both causes and sustains the pattern
- Comorbidity with depression, anxiety, and ADHD is common and clinically important
- In most presentations, problematic use is secondary to an underlying condition
- Avoidance coping is a central and clinically significant pathway to dysregulated use
- Platform design features (variable reinforcement, infinite scroll, algorithmic personalization) are clinically relevant maintaining factors
- CBT has emerging evidence for reducing problematic use and associated symptoms
- The goal of support is controlled, balanced use — not abstinence
- Adolescents are the highest-risk demographic due to developmental factors, not character failing
- Abrupt access restriction in vulnerable adolescents carries risk of acute psychiatric responses
Genuinely uncertain
- Whether internet and social media use dysregulation constitutes a distinct disorder or a symptom cluster
- Whether brain differences observed precede, follow, or interact with the behavioral pattern
- How to define and measure the phenomenon reliably across different populations
- Whether high use in adolescence reflects a self-limiting developmental phase or early disorder
- The long-term trajectory of these patterns across the lifespan
- Whether the same framework applies equally across different types of internet use
- The most effective formats and components of psychological intervention in adult populations
- The specific epidemiology of the access-restriction-as-precipitant phenomenon in adolescents
What helpful support looks like
Cognitive Behavioral Therapy (CBT)
CBT has the strongest evidence base among psychological approaches studied for problematic internet use. It targets the thought patterns and beliefs driving unhelpful behaviors — including those connecting online validation with self-worth — and builds alternative coping strategies and tolerance for unstructured time.
CBT addresses practical behavior change, recognizing high-risk situations and planning for them. Motivational interviewing is useful where ambivalence about change is prominent. Family-based approaches show some of the strongest evidence in younger people and are essential where access restriction is being considered or has been implemented.
Addressing Underlying Conditions
Because problematic internet use is so often connected to underlying mental health conditions — depression, anxiety, ADHD, and others — support frequently works best when those conditions are addressed directly. Effective treatment of an underlying condition often leads to meaningful improvement in the internet use pattern.
Sleep as a Starting Point
Sleep assessment and intervention should be considered a concurrent priority. Given the bidirectional relationship between sleep disruption and dysregulated internet use, behavioral sleep interventions can be initiated independently of other work and may support the regulatory improvements that make use reduction more achievable. Addressing the sleep behavior sometimes makes more progress than addressing the screen behavior directly.
Holding the complexity honestly
The public conversation about internet and social media use tends to move between dismissal and alarm. The research does not support either extreme.
Oversimplification
“Anyone who spends a lot of time online has a problem.”
What the research says
Time spent online is not a reliable indicator of whether use is problematic. The same number of hours may represent necessary engagement, developmentally appropriate social connection, or genuinely impaired regulation. What matters is motivation and functional consequence — not the clock. Adolescents in particular are sometimes pathologized for levels of digital engagement that may reflect developmentally normal behavior.
Oversimplification
“Social media isn’t a real clinical concern.”
What the research says
For a meaningful minority of individuals — estimated at 4–8% of adults and higher in adolescents — the relationship with digital technology becomes genuinely distressing and impairing. The neurobiological substrate for these patterns is real. These experiences deserve to be taken seriously, without either dismissing them as trivial or catastrophizing them as permanent.
Oversimplification
“If internet use is a problem, just take the phone away.”
What the research says
Abrupt, unilateral access removal — particularly in adolescents who are already distressed, who lack alternative social structures, and who have not developed alternative affect regulation strategies — can precipitate acute psychiatric responses including suicidal ideation and self-harm. How access is managed matters enormously. Collaborative, graduated, clinically supported approaches produce better outcomes than unilateral restriction.
Oversimplification
“Brain involvement means the pattern is permanent.”
What the research says
Brain differences associated with problematic internet use are not fixed or permanent. The brain is adaptable, and the patterns observed in research are associated with the behavioral pattern — meaning they can change. Recovery is possible. The difficulty some people experience is real and has a biological dimension — but biological does not mean immutable.
Take Action
Where to go from here
Understanding this area is a beginning, not an endpoint.
If you need help
Resources, support options, and next steps — including guidance for parents concerned about an adolescent's relationship with social media.
For professionals
Clinical resources, assessment frameworks, documentation guidance, and treatment references — including adolescent-specific decision points and access restriction protocols.
For loved ones
Guidance for family members and friends concerned about someone's relationship with digital technology — and how to approach access decisions thoughtfully.
Educational Foundation
Content on this page synthesizes information from peer-reviewed clinical and scientific literature on internet and social media use dysregulation, including neuroimaging research, epidemiological literature, systematic reviews of psychological treatment outcomes, and published clinical frameworks. The nosological positions of DSM-5-TR and ICD-11 are represented accurately as of the time of writing. This field is in active scientific development; findings should be verified against current primary literature for clinical or policy application. This page is intended for educational purposes only and does not constitute clinical guidance. For clinical assessment or treatment, consult a qualified healthcare professional.
Optional Advanced Exploration
Go Deeper — The Clinical Science of Internet & Social Media Use
For readers who want to explore the evidence base, the mechanisms, and the diagnostic debates in greater depth. These modules examine problematic internet and social media use from its definitional foundations through psychology, platform design, comorbidity, and clinical management — territory that is genuinely contested and requires careful navigation. They are optional — the core information above stands on its own.
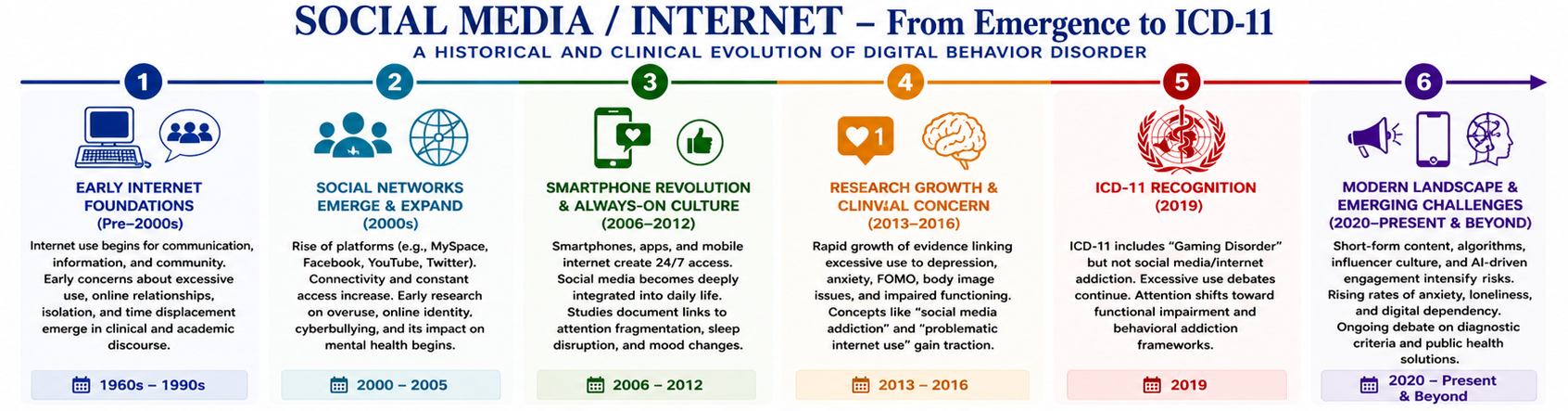
📊 Social Media / Internet – From Emergence to ICD-11: A Historical and Clinical Evolution of Digital Behavior Disorder
Opening Orientation
Why this clinical territory is harder to define than other behavioral conditions — and what an honest engagement with the evidence looks like.
The Definitional Problem
What counts as problematic use when the internet is also a functional necessity? The boundary between heavy engagement, dysregulation, and disorder — and why it remains contested.
Behavioral Phenomenology
Compulsive checking, validation-seeking cycles, FOMO, and the progressive displacement of offline life — what problematic use looks like across different platform contexts.
Psychological Mechanisms
Variable ratio reinforcement, habit formation, mood regulation, identity dependency, and impulsivity — the mechanisms that drive and maintain dysregulated engagement.
Structural & Environmental Drivers
The attention economy, recommendation algorithms, infinite scroll, and notification systems — the deliberately engineered features of the platform environment that shape behavior independently of individual vulnerability.
Psychiatric Comorbidity
Depression, ADHD, social anxiety, and the directional questions that matter most for treatment — why comorbidity is the rule rather than the exception in this population.
Diagnostic Status & Controversy
No formal diagnosis exists for internet or social media use disorder. What that means for clinical practice, coding, and interpreting a prevalence literature ranging from 0.8% to 26.7%.
Clinical Approach & Management
Assessment priorities, CBT adaptations, environmental modification, comorbidity sequencing, and the treatment-goal question that makes this condition distinct from most behavioral addictions.
Synthesis
Integrating biological, psychological, and structural dimensions — and what calibrated clinical practice looks like in a domain where the diagnostic frameworks remain genuinely incomplete.