Gaming Disorder — I’m Trying to Understand
This page is written to inform, not to alarm. Everything here is grounded in current scientific evidence. Where debate exists, it is acknowledged. Where certainty is lacking, that is stated plainly.
Why Understanding Matters
Video games are one of the most widely shared cultural experiences of the modern era. Billions of people play them — across ages, countries, and walks of life. For most, gaming is a source of entertainment, creative challenge, and genuine social connection. It is a normal and often enriching part of contemporary life.
Yet in a small minority of individuals, gaming shifts from something that enriches life to something that begins to consume it. When that shift involves loss of control, persistent harm, and the displacement of other important areas of life, it may meet the criteria for Gaming Disorder — a formally recognized condition in international health systems.
Understanding Gaming Disorder clearly matters for several reasons. Overreacting to gaming — treating all heavy play as pathological — creates unnecessary stigma and can harm young people who are simply enthusiastic hobbyists. Underreacting — dismissing concerns because “it’s just a game” — can delay support for individuals who are genuinely struggling. Accurate understanding allows families, clinicians, educators, and policymakers to respond with appropriate nuance: neither alarmist nor dismissive, but well-informed.
The goal of this page is to offer that grounded understanding.
What Is Gaming Disorder?
Gaming Disorder is a condition defined by a pattern of gaming behavior that involves impaired control, progressive prioritization of gaming over other life domains, and continuation of gaming despite its negative consequences — and that results in significant impairment in a person’s personal, social, educational, or occupational functioning.
Two major international health bodies have formally described this condition, though they have reached somewhat different institutional conclusions.
The World Health Organization (WHO) included Gaming Disorder as a fully recognized diagnosis in the eleventh edition of the International Classification of Diseases (ICD-11), which came into clinical effect in January 2022. Under ICD-11 code 6C51, Gaming Disorder is classified within the Disorders Due to Addictive Behaviours block, alongside Gambling Disorder. The WHO framework identifies three core criteria, all of which must be present: impaired control over gaming; progressive prioritization of gaming over other interests and activities; and continuation of gaming despite negative consequences. The pattern must typically be present for at least twelve months, though a shorter duration may suffice when symptoms are severe, and must result in significant distress or functional impairment.
The American Psychiatric Association (APA) has taken a more cautious position. In the DSM-5-TR, the condition is listed in Section III under the name Internet Gaming Disorder, as a condition requiring further research before formal diagnostic recognition can be granted. The APA framework identifies nine proposed criteria, five or more of which must be endorsed, and includes features such as tolerance, withdrawal-like mood states, preoccupation, deception, and escapism alongside the core features of impaired control and functional harm. The APA’s caution reflects ongoing scientific debate about how to reliably distinguish the disorder from intensive non-pathological play, how to weigh individual criteria, and how well the current evidence generalizes across cultures.
Key distinguishing features
Despite their differences in institutional status, both frameworks converge on one essential point: the functional impairment requirement. Gaming Disorder is not defined by how many hours a person plays. It is defined by whether gaming is causing real harm to their ability to function in daily life. This distinction is foundational to everything that follows.
- Loss of control over gaming — difficulty stopping despite trying
- Gaming crowds out other valued activities and responsibilities
- Continuation despite visible negative consequences
- Pattern present for at least 12 months (or less if severity warrants)
- Significant distress or functional impairment in daily life
- Dysphoric mood states (irritability, restlessness) when unable to play
- Using gaming as a primary coping mechanism for negative emotions
- Not explained by heavy engagement or recreational dedication alone
Not all features are present in every individual, and severity can vary.
The Spectrum of Gaming Involvement
Gaming behavior exists on a continuum. The vast majority of people who play games — including those who play frequently and for extended periods — fall well within the healthy end of that spectrum.
Recreational gaming
Describes the experience of most players: gaming as a leisure activity pursued for enjoyment, relaxation, competition, or social interaction. Even extensive recreational gaming is not a problem if a person maintains control over when they play, sustains their responsibilities, and retains their other interests and relationships.
High engagement
Refers to a more intensive relationship with gaming — the dedicated hobbyist, the competitive player, the person for whom gaming is a central and deeply meaningful pursuit. High engagement may involve long sessions, significant investment of time, and genuine passion for the activity. It is not pathological. Many highly engaged gamers are also professionally and socially functional, with rich lives outside of gaming.
At-risk or problematic gaming
Describes a pattern where warning signs are beginning to emerge — increasing difficulty stepping away, some early slippage in responsibilities, using gaming as the primary way to manage stress or negative emotion — but the full clinical threshold for disorder has not been met. This is a zone worth paying attention to, particularly in adolescents, but it does not constitute a diagnosis.
Gaming Disorder
Represents the far end of the spectrum: a clinically significant pattern of impaired control, displaced priorities, and continued gaming despite demonstrable harm, causing meaningful disruption to the person’s life. This affects a small minority of gamers.
Movement along this spectrum is possible in both directions. Many individuals who develop problematic gaming patterns recover — sometimes through professional support, sometimes through natural life changes. The spectrum is not a one-way progression.
The Neuroscience of Gaming Disorder
Neurobiological research has made meaningful progress in understanding Gaming Disorder, though it remains methodologically early-stage and should be interpreted with appropriate caution. Current evidence draws primarily on structural and functional brain imaging, neuropsychological assessment, and inference from related behavioral addiction research.
The brain’s reward system plays a central role in Gaming Disorder. Video games — particularly those designed around variable reward schedules, achievement systems, and social reinforcement — are highly effective at activating the dopaminergic pathways associated with motivation, anticipation, and pleasure. Over time, in individuals who develop Gaming Disorder, there is evidence of altered neural responses to gaming-related cues: heightened activation in areas associated with anticipatory cognition and self-referential processing, and reduced activation in areas associated with self-regulation and impulse control.
Structural brain imaging studies have identified gray-matter volume differences in regions involved in decision-making, impulse control, and reward processing in individuals with Gaming Disorder. Notably, the specific neurobiological pattern observed in Gaming Disorder is not identical to that seen in Substance Use Disorders — in particular, the robust striatal hyperactivation characteristic of substance addiction is not consistently found in Gaming Disorder research. Whether this reflects a genuinely distinct neurobiological mechanism, or simply reflects the earlier and more limited state of the evidence base, remains an active question.
Impulse control is a consistent area of difference in neuropsychological studies: individuals with Gaming Disorder demonstrate performance deficits on tests of inhibitory control, working memory, and decision-making under uncertainty. These deficits parallel findings in other behavioral addictions, though the interpretive challenge of whether such differences represent predisposing traits or consequences of the disorder itself has not been resolved.
A central mechanism sustaining gaming in disordered users appears to be the partial reinforcement effect: intermittent and unpredictable reward delivery produces stronger and more persistent behavioral patterns than predictable reward. This principle is architecturally embedded in many contemporary game designs, which is one reason the online and multiplayer gaming environment represents a particularly potent context.
Developmental context matters significantly here. The prefrontal systems that govern impulse control and long-term decision-making continue maturing through the mid-twenties. Adolescents are neurobiologically more vulnerable to reinforcement-driven behavior patterns and less equipped with the regulatory resources that help adults modulate compulsive tendencies. This is one reason adolescence represents a period of elevated risk.
All neurobiological findings in this area are based predominantly on cross-sectional studies with relatively small and culturally concentrated samples. Causal relationships between brain changes and disorder development cannot be established from existing data.
Risk Factors and Protective Factors
Gaming Disorder does not arise in a vacuum. A range of individual, psychological, social, and environmental factors influences who is more or less vulnerable.
Individual and psychological risk factors
Include impulsivity and difficulty with self-regulation, which are among the most consistently documented individual-level predictors. Attention-Deficit/Hyperactivity Disorder (ADHD) is the most robustly documented psychiatric vulnerability, with individuals with ADHD showing substantially elevated rates of Gaming Disorder and longitudinal evidence suggesting that inattention specifically predicts disorder development over time. Depression and anxiety — including social anxiety in particular — are also strongly associated, with evidence supporting bidirectional relationships: these conditions may drive a person toward gaming as a form of escape, while disordered gaming may in turn deepen depressive and anxious symptoms. Low frustration tolerance, avoidant coping styles, and social difficulties round out the individual risk profile.
Social and environmental risk factors
Include social isolation, poor peer relationships, and family conflict — particularly emotional unavailability or excessively restrictive parenting. For some individuals, online gaming environments fill a genuine social void, creating a situation where digital social worlds substitute for the real-world connection that is absent or inaccessible. Early and unsupervised exposure to high-engagement gaming in childhood may also contribute.
Online ecosystem factors
Are not trivial. Game designs that incorporate continuous variable reinforcement, social obligation mechanics (such as guild commitments or team-based scheduling demands), and in-game economies create environments with genuine engagement and retention pressure. These design features do not cause disorder on their own, but they interact with individual vulnerabilities in ways that can amplify risk.
Protective factors
Include strong real-world social support, a diverse range of meaningful activities and interests outside of gaming, healthy sleep habits, stable family relationships, and the presence of clear and consistent structure. The ability to use gaming for genuine recreation — enjoyment without compulsion — while maintaining other life domains appears to be a meaningful marker of healthy engagement.
Consequences Across Life Domains
When Gaming Disorder is present, its consequences tend to be visible across multiple areas of life simultaneously.
Academic and occupational functioning
Is commonly affected. Declining grades, missed assignments, reduced attendance, and eventual academic disengagement are well-documented in adolescent presentations. For adults, impaired concentration, reduced productivity, and difficulties meeting work obligations have been reported. The gradual displacement of educational and occupational investment by gaming is a hallmark pattern.
Sleep
Is one of the most consistently affected domains. Nocturnal gaming — playing through the night or into the early morning hours — disrupts circadian rhythms, reduces total sleep duration, and impairs daytime alertness and cognitive function. Sleep disturbance is both a consequence of Gaming Disorder and a factor that worsens mood, impulse control, and concentration, creating a reinforcing cycle.
Social and interpersonal functioning
Is often profoundly affected. Family conflict over gaming is common, and real-world friendships and romantic relationships frequently deteriorate as gaming crowds out shared time and emotional presence. A clinically important complexity is that for some affected individuals, online gaming communities represent their primary social environment — which means that treatment approaches that focus exclusively on reducing gaming must also address the social scaffolding that gaming has come to provide.
Emotional and psychological wellbeing
Is commonly compromised. Dysphoric mood states — irritability, anxiety, restlessness, and low mood — occur both during periods of enforced gaming abstinence and more persistently as the disorder deepens. Many individuals use gaming as a primary coping mechanism for stress and negative emotion, a pattern that provides short-term relief while deferring engagement with the underlying emotional difficulty.
Physical health
consequences reflect the behavioral profile of extended sedentary engagement with disrupted self-care: sleep disruption, poor nutrition, reduced physical activity, and musculoskeletal complaints including neck, shoulder, and wrist strain. These are not as severe or as systematic as the physical sequelae of substance use disorders, but they are clinically real.
Common Myths
Anyone who plays games for many hours is addicted.
This is not correct. Duration of play, by itself, is neither a diagnostic criterion nor a reliable indicator of disorder. Many individuals play for extended hours without any loss of control, functional impairment, or clinical concern. The defining feature of Gaming Disorder is impaired control combined with real-world harm — not the number of hours logged.
Gaming Disorder is just laziness or a lack of willpower.
This framing misrepresents the condition and is harmful. Gaming Disorder involves documented alterations in the brain systems governing impulse control and reward processing. It is frequently comorbid with ADHD, depression, and anxiety — conditions that themselves affect self-regulation. Reducing it to a character flaw obscures the genuine clinical picture and discourages people from seeking help.
Only teenagers are affected.
Adolescents and young adults do represent the demographic group at highest risk, and most research has focused on this population. However, Gaming Disorder occurs across the adult lifespan, including in individuals who were recreational gamers for years before developing disordered patterns in adulthood. The disorder does not have an age ceiling.
Gaming itself causes the disorder.
The vast majority of people who game — including those who do so intensively — do not develop Gaming Disorder. Gaming is not inherently pathological any more than exercise is inherently exercise addiction. What matters is the individual’s relationship with the activity, their capacity to regulate it, and whether it is functionally impairing their life.
Nothing can be done about it.
There are effective approaches. Cognitive behavioral therapy has demonstrated meaningful outcomes across multiple clinical studies. Family-based interventions improve outcomes particularly for younger patients. Addressing co-occurring psychiatric conditions often produces secondary benefits for gaming behavior. Many individuals also recover through natural life changes and supported habit restructuring. Recovery is possible and, for many, achievable.
Prevalence and Epidemiology
Estimating the true prevalence of Gaming Disorder is genuinely difficult, and figures in the published literature vary considerably. This variance reflects real methodological challenges: the diagnostic criteria were not internationally standardized until 2022, different studies have applied different instruments and thresholds, and many early studies used self-selected online samples that tend to produce inflated estimates.
Studies applying rigorous diagnostic criteria — including the functional impairment requirement — in representative population samples consistently report lower prevalence figures than earlier, less methodologically stringent research. The best available evidence suggests that Gaming Disorder affects a small minority of gamers: general population estimates in adolescent and young adult samples fall roughly in the range of one to five percent when impairment criteria are applied carefully. The disorder is more common than in the general public among individuals already presenting with depression, ADHD, or anxiety, given the overlapping vulnerability pathways.
Gaming Disorder is more prevalent in males than females across all study populations and regions, with the difference most pronounced in certain gaming genres (first-person shooters, in particular) and somewhat narrowed in others (role-playing games). The demographic peak occurs in adolescence and young adulthood, with risk generally declining through the late twenties, though longitudinal studies confirm that disorder classification can persist meaningfully over time rather than resolving spontaneously in all cases.
Geographic variation is a notable feature of the literature, with consistently elevated estimates from East Asian samples — particularly South Korea and China — relative to Western populations. Whether this reflects genuine cultural differences in gaming norms and practices, methodological factors related to early and intensive research activity in these regions, or other variables is not fully resolved.
The essential takeaway is that most people who game, including most who game frequently, are not affected by Gaming Disorder. The disorder is real, but it is not common.
Recovery Is Possible
One of the most important messages this page can offer is that recovery from Gaming Disorder is achievable for most individuals who seek and receive appropriate support.
Cognitive Behavioral Therapy (CBT)
Is the most extensively studied psychological approach and represents the current reference intervention. CBT helps individuals identify and challenge the thinking patterns that sustain compulsive gaming, develop alternative coping skills for managing stress and negative emotions, engage in behavioral activation toward rewarding non-gaming activities, and build relapse prevention plans. Evidence supports meaningful improvement in gaming disorder symptoms, depression, anxiety, social functioning, and impulse control through CBT.
Family-based approaches
Are particularly relevant for adolescent presentations and for adults in significant relationships. Supportive, non-confrontational family involvement — as opposed to abrupt restriction or high-conflict confrontation — generally produces better engagement and outcomes. Gaming may have become the person's primary social space, and treatment planning that accounts for this reality tends to be more effective than approaches that simply remove the behavior without addressing the social need it was meeting.
Addressing co-occurring conditions
Is often central to treatment success. In many individuals, depression, anxiety, or ADHD are primary drivers of the gaming pattern. Effectively treating these conditions — through therapy, medication, or both — frequently produces secondary improvement in gaming behavior. Treatment for Gaming Disorder should routinely include comprehensive evaluation and management of psychiatric comorbidities.
Treatment goals
Are typically oriented toward restoring balance rather than achieving complete abstinence. Since most affected individuals need access to computers and digital devices for education and work, a harm-reduction model — returning gaming to a manageable role in life rather than eliminating it entirely — is often more realistic and more acceptable to the individual. Some individuals may choose abstinence from specific games or genres that have been most problematic; this is a clinical decision guided by individual circumstances.
Natural recovery occurs: some individuals who have experienced problematic gaming patterns resolve them through life transitions, changing circumstances, or their own deliberate effort without formal clinical intervention. This should neither be used to dismiss the seriousness of the disorder nor to discourage those who need support from seeking it.
Similarities and Differences with Substance Use Disorders
The classification of Gaming Disorder within addictive disorders frameworks reflects genuine neurobiological and behavioral parallels with substance use disorders — but also meaningful differences that warrant clear communication.
Similarities
Are substantive. Both Gaming Disorder and substance use disorders involve dysregulation of the brain’s reward and motivation systems, with evidence of dopaminergic pathway involvement in both. Both involve impaired control over a behavior despite negative consequences. Both demonstrate patterns of escalating engagement over time, in at least some affected individuals, that parallel tolerance dynamics in substance dependence. Both involve preoccupation with the behavior, continued engagement despite harm, and mood-related cravings or urges to engage. Both show elevated co-occurrence with depression, anxiety, and ADHD. These structural parallels are why the behavioral addiction framework — originally developed for Gambling Disorder — extends meaningfully to Gaming Disorder.
Differences
Are equally important. Gaming Disorder involves no ingestion of a psychoactive substance. There is no pharmacological intoxication, and there is no physiological withdrawal syndrome comparable to that seen with alcohol, opioids, or benzodiazepines. The dysphoric mood states that arise when a person with Gaming Disorder stops or reduces play — irritability, restlessness, low mood, anxiety — are psychologically real and clinically significant, but they are affective and behavioral in nature rather than physiological. This distinction matters for clinical assessment, for patient communication, and for understanding the mechanism of the disorder.
Additionally, current neuroimaging evidence suggests that Gaming Disorder may differ neurobiologically from substance use disorders in specific ways — most notably, the robust striatal hyperactivation to drug-related cues that reliably characterizes addiction neuroscience findings in substance dependence has not been consistently replicated in Gaming Disorder research. Whether this represents a genuinely distinct mechanism or a limitation of the current evidence base is an open question.
The behavioral addiction model — common reward pathway involvement, impaired control, reinforcement-driven behavior, functional harm — is the most appropriate conceptual frame for understanding Gaming Disorder. It should neither be conflated with substance dependence nor dismissed as categorically different from the phenomenon that framework describes.
Cultural and Environmental Context
Gaming is a genuinely global activity, and the cultural context in which it occurs shapes both the experience of gaming and the nature and prevalence of related disorders in ways that the field is only beginning to understand.
The rapid and near-universal proliferation of gaming technology —
Particularly mobile gaming, which has made gaming accessible in virtually every context and at every income level — means that Gaming Disorder is an emerging clinical concern in settings where it was previously invisible. The social ecosystems built around online gaming communities, particularly massively multiplayer online environments, create contexts in which gaming is not simply an individual activity but a social identity, an economy, and a set of commitments and obligations. For many adolescents and young adults, online gaming communities represent genuine social worlds with meaningful relationships, shared language, and collective purpose. This social dimension is clinically relevant both as a risk factor (the difficulty of leaving a meaningful social community) and as a treatment consideration.
Game design practices —
Including variable reward systems, achievement progression, social obligation mechanics, and monetization features that tie real-world spending to in-game rewards — are relevant environmental factors. These design elements are not inherently pathological, and they are engaged by billions of players without clinical consequence. However, they interact with individual vulnerability in ways that can amplify risk for those already predisposed to impaired control over rewarding behaviors.
Geographic variation in prevalence —
With consistently higher estimates from East Asian populations, particularly South Korea and China — has prompted genuine scientific debate about whether diagnostic thresholds developed primarily in Western research contexts are fully applicable across cultures, whether different cultural norms around gaming intensity and esports participation create different relationships between play and harm, and whether the concentration of Gaming Disorder research in certain regions creates a sampling artifact. These are unresolved questions, and they are important ones for both clinical practice and policy.
There is also an active scientific debate about overdiagnosis —
The concern that a moral or cultural panic about screen time and gaming could lead to pathologizing normal intensive engagement, particularly in young people for whom gaming is a central cultural medium. This concern is legitimate and is best addressed by rigorous application of the functional impairment criterion. The disorder, properly diagnosed, requires demonstrable real-world harm. Without that, no diagnosis is warranted.
Prevention Approaches
Preventing Gaming Disorder does not mean preventing gaming. It means cultivating the conditions in which gaming is more likely to remain a healthy part of life rather than becoming a source of harm.
Healthy digital habits —
A phrase that sounds simple but requires active cultivation — include maintaining a diverse range of activities outside of gaming, preserving real-world social relationships, protecting sleep by establishing boundaries around nighttime gaming, and developing conscious awareness of one's own relationship with gaming over time. Teaching young people to notice when play stops feeling like choice and starts feeling like compulsion is a meaningful preventive skill.
Parental engagement
Is most effective when it is involved and curious rather than restrictive and conflictual. Understanding what a child or adolescent is actually doing in gaming environments — who they play with, what draws them to particular games, what needs gaming is meeting — provides a foundation for more effective guidance than blanket time limits or device removal. When limits are established, they are more effective when collaborative and consistent. That said, maintaining some structure around gaming — particularly around sleep — is genuinely protective.
School-based education
Can build media literacy and critical awareness of how digital environments, including games, are designed to sustain engagement. Teaching young people to understand reinforcement design, to recognize early warning signs in their own behavior, and to value a range of activities provides a resilience foundation.
Early intervention
Matters. When a young person's gaming pattern is beginning to cause visible problems — slipping grades, social withdrawal, disrupted sleep — early and supportive conversation is more effective than waiting for the situation to escalate. The goal of early intervention is not to stigmatize or pathologize the behavior but to restore balance before impairment deepens.
Policy considerations
In this area are active and evolving. Regulatory discussions about game design practices, particularly around variable reward mechanics and in-game purchasing systems, are ongoing in multiple jurisdictions. These conversations are worth monitoring, but they are best approached with the same epistemic caution that characterizes this field overall: the evidence base for specific policy interventions is still developing.
Where to Go From Here
Understanding Gaming Disorder is a beginning, not an endpoint. Where you go from here depends on why you came.
If you are concerned about your own gaming:
It can be valuable to reflect honestly on whether gaming is affecting areas of your life that matter to you — your relationships, your work or studies, your sleep, your ability to do things you used to care about. If the answer is yes, and if you have noticed that cutting back has been harder than expected, speaking with a mental health professional is worth considering. A qualified clinician can help you understand what is happening and what, if anything, might help.
If you are concerned about someone you care for:
Concern is more effective when it is curious and open rather than accusatory. If someone in your life appears to be struggling with gaming, expressing concern honestly and without contempt — and, when the time is right, supporting them in speaking with a professional — is more likely to help than conflict or ultimatum. Families benefit from professional guidance too, and family-based approaches have some of the strongest evidence in this field.
If you are a professional or researcher:
The clinical resources and professional synthesis materials associated with this platform offer a more technically detailed orientation to the evidence base, diagnostic frameworks, assessment instruments, and treatment considerations. The field is evolving rapidly, and the available literature carries methodological limitations that require careful interpretation.
If you are a journalist, educator, or policymaker:
The most important contribution you can make to public discourse on this topic is accuracy. Gaming Disorder is a real clinical phenomenon affecting a minority of gamers — it is not a mass crisis, and it is not a moral failing. Covering it with the same rigor and nuance applied to other health topics serves both the public and the individuals whose experiences are at stake.
Curiosity about this topic is valuable — whether for understanding, for concern, or for professional purpose. This resource will be here whenever you want to return.
Optional Advanced Exploration
Go Deeper — The History & Science of Gaming Disorder
For readers who want to explore the full historical arc, the development of diagnostic thinking, and the evidence base in greater depth. These modules trace gaming disorder from its earliest cultural roots through neuroscience, contested classification, and the modern digital landscape. They are optional — the core information above stands on its own.
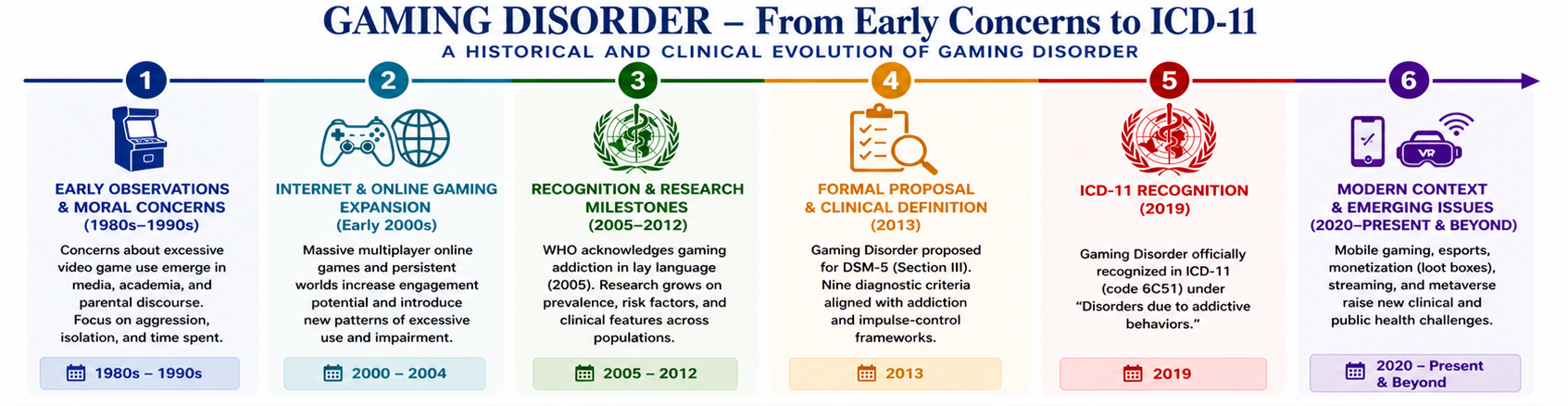
📊 Gaming Disorder – From Early Concerns to ICD-11: A Historical and Clinical Evolution
Opening Orientation
Why gaming disorder matters — and what a historically informed clinical perspective adds to understanding it.
Origins of Play & Competition
The deep roots of structured play — from ancient games to early arcade culture and the emergence of video gaming as a mass phenomenon.
Cultural & Social Integration
How gaming became embedded in social life — the rise of gaming identity, community, esports, and the normalization of intensive play.
Technological Transformation
From console to internet to mobile — how each technological shift expanded access, altered engagement patterns, and changed the risk landscape.
Institutionalization & Industry Expansion
The growth of a global industry — how commercial gaming design, monetization mechanics, and platform ecosystems shaped both engagement and harm.
Moralization & Early Psychopathology
The early clinical and cultural response — moral panics, first case reports, and the gradual shift from behavioral concern to psychiatric inquiry.
Diagnostic Recognition: DSM-5 to ICD-11
The formal classification history — from Internet Gaming Disorder in DSM-5 Section III to full ICD-11 recognition, and the scientific debate that shaped both.
Treatment: What the Evidence Actually Supports
CBT, family-based approaches, addressing comorbidities — what works, what is emerging, and what the current evidence base genuinely supports.
Synthesis: The Biopsychosocial Framework
Integrating biological, psychological, social, and technological dimensions into a coherent clinical understanding of gaming disorder.